Expertise: Investigative journalism, editing, start-ups, content and magazine design, digital content, digital strategy.
Locations: Toronto and Guelph, Ontario, Canada and London, UK 1991 to 1997
Investigative Journalist, Editor, Reporter, Writer: David South
Abstract
I worked as a journalist for magazines and newspapers from 1991 to 1997 in Canada and the United Kingdom and as a radio host for a weekly spoken word interview programme, Word of Mouth (CKLN-FM).
This included working as an investigative journalist for Now Magazine, “Toronto’s alternative news and entertainment source”, as a Medical and Health Correspondent for Today’s Seniors, and as an investigative journalist and reporter for two Financial Times newsletters, New Media Markets and Screen Finance.
Samples of published stories can be found here (below) and on the Muck Rack platform here: https://muckrack.com/david-south
About
Could it be possible to do high-quality investigative journalism in the context of a shrinking economy undergoing austerity, and where the media sector is contracting and consolidating around a small number of media companies? Is it possible to launch new media products in the face of a contracting economy and reach new audiences and create new markets?
In Canada, the early to mid 1990s were the years of government austerity and economic crisis. After the crash of 1989/1990*, institutions came under great stress. Health care, for example, was pitched into a period of turmoil and change. Drawing on my experience working in the health sector (Princess Margaret Hospital/Ontario Cancer Institute), I covered this crisis in many stories for various publications, in particular Today’s Seniors.
The Canadian economy severely contracted and unemployment was at 11.4 per cent by 1993 (Statistics Canada), and as Statistics Canada says, “Because employment recovered at a snail’s pace after the recession of the early 1990s, the decline in the unemployment rate was delayed until 1994”.
The media in general could not avoid the wider economic crisis. According to the book The Missing News: Filters and Blind Spots in Canada’s Press (Robert A. Hackett and Richard S. Garneau, Canadian Centre for Policy Alternatives, University of Toronto Press 2000), Canada’s media was also in a crisis throughout the 1990s, as declining resources, staff layoffs and media closures reduced the breadth and depth of news coverage. Canadian media as a whole also has a “great dependence on advertising, which accounts for more than 70% of daily newspaper revenues, about 64% of magazine revenues,” which means there is enormous pressure to only publish stories that do not upset advertisers. And monopolies exert great control over news content in Canada: “In the United States, ten companies control 43.7% of total daily newspaper circulation. By contrast, in Canada since 1996, one single company controls a comparable share of the media pie.”
The impact of this crisis was summed up by Jeffrey Simpson in the book The Missing News, where he said newspapers are “shrinking in size, personnel, ambition and, as a consequence, in their curiosity,” …. “I believe the result has been a diminution in quality.” (p64)
This is the context in which, ironically, it was possible to flourish as a much-sought-after investigative journalist who could get the story and get the quotes and as an editor. And it was also a time for opportunity, in particular as new media rose in importance, from cable and satellite television, to the rise of the Internet.
I broke original stories for Now Magazine as a member of their investigative reporting team, for Today’s Seniors as its Medical and Health Correspondent, and as a reporter for two Financial Times newsletters in London, UK. I also broke original stories as a freelancer for many other magazines and newspapers, including Hospital News, The Toronto Star, This Magazine, The Annex Gleaner, Flare, The Financial Post Magazine, Canadian Living, and others. I drew on strong contacts in health care, media, politics, international relations and the military.
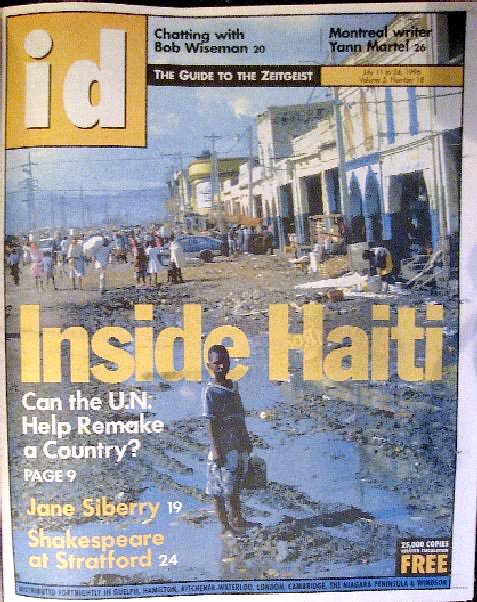
I was an editor for magazines, newspapers and newsletters as well, gaining invaluable experience and contacts. This included as Editor-in-Chief for start-up youth publication, Watch Magazine (see Case Study 2), and as Features Editor for Id Magazine (see Case Study 3).
Themes covered included the uses – and abuses – of data, the impact of military engagements to uphold international law, how to re-structure health care when budgets are tight, with populations ageing, and technology and scientific advances quickly expanding options, the emerging new media world of cable and satellite television and the Internet, the sexual revolution 2.0, urbanization and how it re-shapes politics and community, international development, and youth culture.
Story highlights include covering data concerns over Canada’s border screening measures, questions about the air quality of aircraft cabins, the debate over airstrikes in Bosnia, scandals involving peacekeepers in Somalia and reporting on the UN peacekeeping mission in Haiti, reforms to medical education in Canada, innovators in health care, the tug of war over health care spending during austerity measures, London, UK designers, the growing role of Nordic countries in cable and satellite television, the film financing scene in Europe and the UK, the new sexual revolution and its impact on cable and satellite television and the rising Internet, changes to Canada’s media industry, and Toronto’s embracing of the megacity concept and the political battles it sparked.
I edited newsletters and newspapers aimed at specific communities, from Canada’s medical history community to part-time students. And had the privilege of helming a start-up youth magazine as its Editor-in-Chief to its commercial success (see Case Study 2).
It was an exciting time of great change, best reflected by the fact in 1997 Id Magazine (Features Editor: see Case Study 3) was one of the first Canadian publications to regularly publish an online version (https://web-beta.archive.org/web/19970207103121/www.idmagazine.com).
* “The last two recessions in Canada occurred in 1982 and 1990. … The most recent Canadian recession began in the second quarter of 1990 and over the next 12 months GDP fell by 3.2%. … The recovery from this recession was unusually slow; there was almost no growth between mid-1991 and mid-1992. This slow recovery was export driven.” (The Canadian Encyclopedia)
“In early 1994, Canada’s economic situation was not that favourable—our economy was facing some rather serious problems.
“… the recession here was more severe than in the United States.
“Working their way out of these difficulties was disruptive and painful for Canadian businesses. Defaults, restructurings, and downsizings became the order of the day. With all this, unemployment took a long time to recover from the 1990–91 recession and, in many instances, wages and salaries were frozen or reduced (Bank of Canada: Canada’s Economic Future: What Have We Learned from the 1990s?)
A small sample of published stories with links is below:
Investigative Journalism
Aid Organization Gives Overseas Hungry Diet Food
Artists Fear Indifference From Megacity
Casino Calamity: One Gambling Guru Thinks The Province Is Going Too Far
False Data Makes Border Screening Corruptible
New Student Group Seeks 30 Percent Tuition Hike
Peaceniks Questioning Air-raid Strategy in Bosnia
Somali Killings Reveal Ugly Side of Elite Regiment
Top Reporters Offer Military Media Handling Tips
Will the Megacity Mean Mega-privatization?
Will Niagara Falls Become the Northern Vegas?
Health and Medical
Changing Health Care Careers a Sign of the Times
Critics Blast Government Long-Term Care Reforms
Cut Services to Elderly, Says Doctors’ Survey … But Leave Our Salaries Alone!
Feds Call for AIDS, Blood System Inquiry: Some Seniors Infected
Government Urged to Limit Free Drugs for Seniors
Health Care on the Cutting Block: Ministry Hopes for Efficiency with Search and Destroy Tactics
New Legislation Will Allow Control of Medical Treatment
New Seniors’ Group Boosts ‘Grey Power’: Grey Panthers Chapter Opens with a Canadian Touch
Philippine Conference Tackles Asia’s AIDS Crisis
Private Firms Thrive as NDP ‘Reinvents’ Medicare
Psychiatric Care Lacking for Institutionalised Seniors
Seniors Falling Through the Health Care Cost Cracks
Specialists Want Cancer Treatments Universally Available
Take Two Big Doses of Humanity and Call Me in the Morning
Taking Medicine to the People: Four Innovators In Community Health
US Health Care Businesses Chasing Profits into Canada
Magazines
The Ethics of Soup: Grading Supermarket Shelves – For Profit
Freaky – The 70s Meant Something
Land of the Free, Home of the Bored
Oasis Has Arrogance, A Pile of Attitude and the Best Album of 1994
Redneck Renaissance: A Coterie of Journalists Turn Cracker Culture into a Leisure Lifestyle
Swing Shift: Sexual Liberation is Back in Style
Media
The Big Dump: CP’s New Operational Plan Leaves Critics with Questions Aplenty
Channel Regulation: Swedes will Fight Children’s Advertising all the Way
Do TV Porn Channels Degrade and Humiliate?
Is the UK Rushing to Watch TV Porn?
Playboy ‘is not for sad and lonely single men’
TV’s Moral Guide in Question – Again
UK Laws on Satellite Porn Among Toughest in Europe
Undercurrents: A Cancellation at CBC TV Raises a Host of Issues for the Future
Special Reports
United Nations
Freedom of Expression: Introducing Investigative Journalism to Local Media in Mongolia
Starting from Scratch: The Challenge of Transition
State of Decay: Haiti Turns to Free-market Economics and the UN to Save Itself
Traffic Signs Bring Safety to the Streets
Magazines
Newsletters
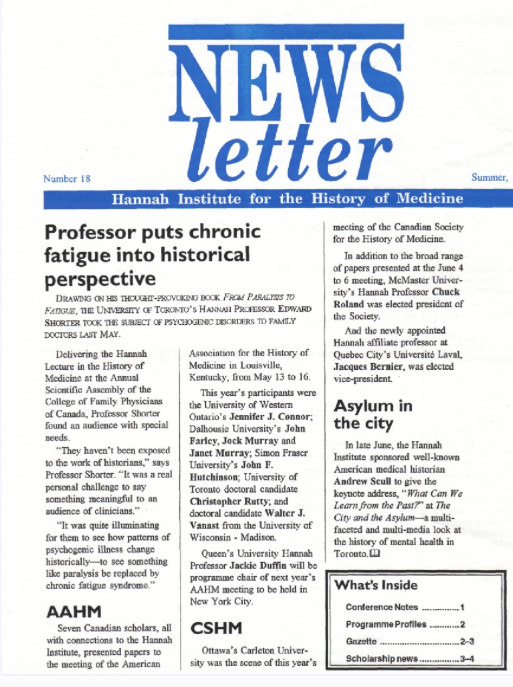
Hannah Institute for the History of Medicine
Other Resources
In Their Own Words: Selected Writings by Journalists on Mongolia, 1997-1999 (ISBN 99929-5-043-9)
Mongolian Rock and Pop Book (ISBN 99929-5-018-8)
Wild East: Travels in the New Mongolia (ISBN 1-55022-434-4)
Timeline
1991: Begin career as investigative journalist and editor.
1992: Work as a Medical and Health Reporter for Today’s Seniors and as an Investigative Journalist for Now Magazine. Work as Editor and Writer for the Hannah Institute for the History of Medicine’s newsletter.
1993: Published in many publications, including The Toronto Star, Canadian Living and This Magazine.
1994: Work on re-launch of Watch Magazine 2.0 and its expansion (see Case Study 2).
1995: Work as reporter for two Financial Times newsletters in London, UK.
1996: Work on re-launch of Watch Magazine 3.0 and its expansion. Begin work at Id Magazine as its Features Editor (see Case Study 3).
1997: Begin two-year assignment with the United Nations mission in Mongolia (see Case Study 4).
Testimonials
“David South … proved himself to be a penetrating, thorough and hard-working journalist. He produced a lot of very good stories …” Neil McCartney, Editor, Screen Finance, Telecom Markets and Mobile Communications, London, UK



This work is licensed under a Creative Commons Attribution 4.0 International License.
ORCID iD: https://orcid.org/0000-0001-5311-1052.
© David South Consulting 2025



You must be logged in to post a comment.