The idiosyncracies of Canada’s medical schools can be both a strength and a drawback. An exchange program sponsored by the Hannah Institute hopes to bring the schools a little closer by opening up the communication lines from coast to coast.
The first exchange took place this April between the University of Western Ontario and the University of Calgary. Medical students met at Western for three days of talks and socializing.
“One of the objectives is to have each student work up a talk of ten minutes to stimulate further research,” says UWO Hannah Professor Paul Potter, who helped coordinate the exchange along with Calgary’s Dr. Peter Cruse.
Topics ranged from diseases among the Cree of Alberta to the old medical art of uroscopy.
Professor Potter says he hopes the exchange will become a regular annual affair, possibly with next year’s exchange matching Calgary with Halifax’s Dalhousie University.
I worked as Editor and Writer for the newsletter of the Hannah Institute for the History of Medicine (under the direction of the Editor-in-Chief and Hannah Executive Director Dr. J.T. H. Connor) in the early 1990s. Located close to the University of Toronto and within a neighbourhood claiming a long association with medical and scientific discovery (Sir Frederick Banting, co-developer of insulin for the treatment of diabetes, lived at 46 Bedford Road,), the goal was to better connect Canada’s medical history community of scholars and raise the profile of the funding resources available to further the study of medical history in Canada.
“… in recent years it has become a pursuit for a growing number of researchers. … Behind much of this growth has been the Hannah Institute for the History of Medicine which has encouraged writing …”.
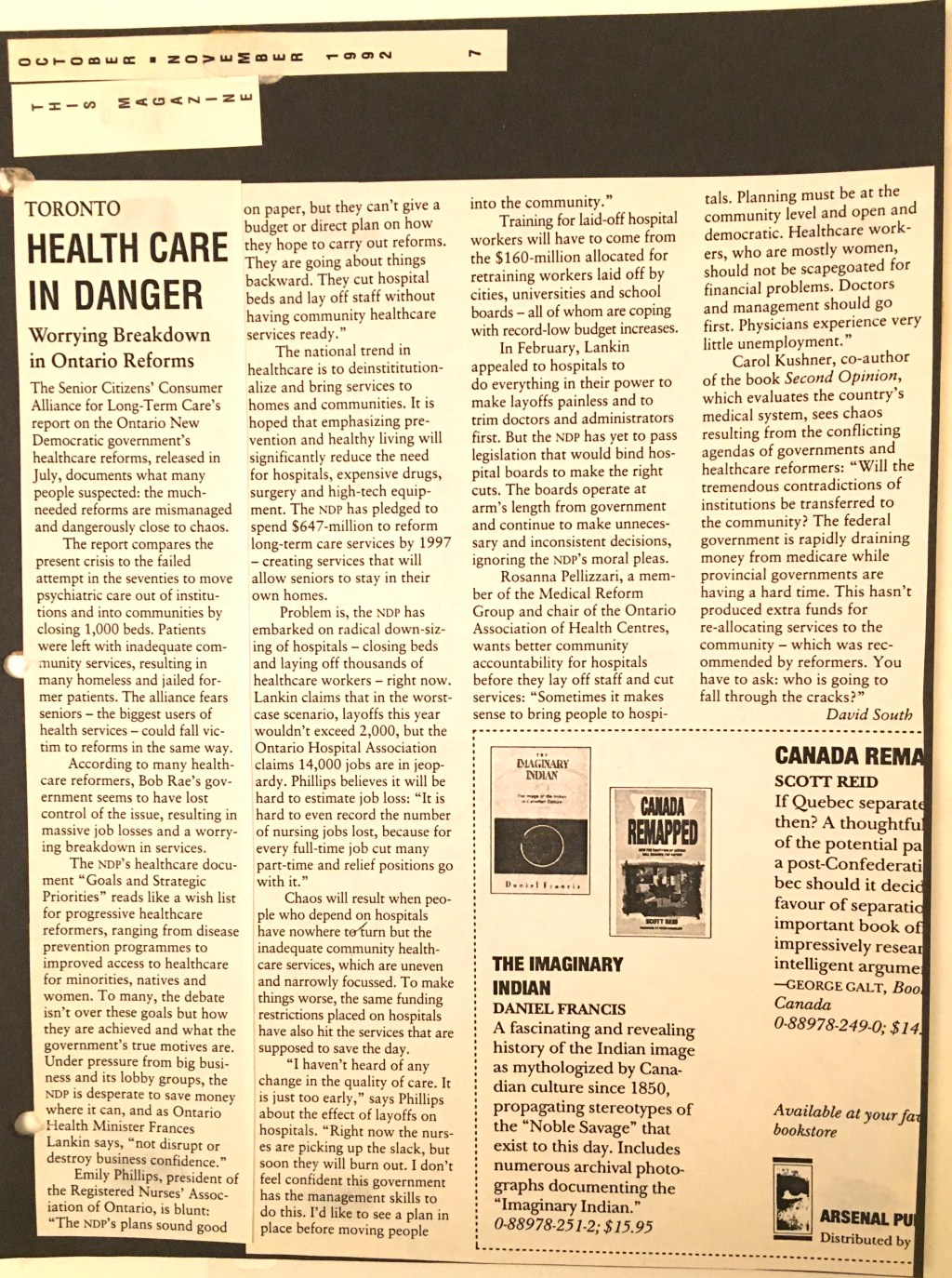
The Senior Citizens’ Consumer Alliance for Long-Term Care’s report on the Ontario New Democratic government’s health care reforms, released in July, documents what many people suspected: the much-needed reforms are mismanaged and dangerously close to chaos.
The report compares the present crisis to the failed attempt in the seventies to move psychiatric care out of institutions and into communities by closing 1,000 beds. Patients were left with inadequate community services, resulting in many homeless and jailed former patients. The alliance fears seniors – the biggest users of health services – could fall victim to reforms in the same way.
According to many health care reformers, Bob Rae’s government seems to have lost control of the issue, resulting in massive job losses and a worrying breakdown in services.
The NDP’s health care document “Goals and Strategic Priorities” reads like a wish list for progressive health care reformers, ranging from disease prevention programmes to improved access to health care for minorities, natives and women. To many, the debate isn’t over these goals but how they are achieved and what the government’s true motives are. Under pressure from big business and its lobby groups, the NDP is desperate to save money where it can, and as Ontario Health Minister Francis Lankin says, “not disrupt or destroy business confidence.”
Emily Phillips, president of the Registered Nurses’ Association of Ontario, is blunt: “The NDP’s plans sound good on paper, but they can’t give a budget or direct plan on how they hope to carry out reforms. They are going about things backward. They cut hospital beds and lay off staff without having community health care services ready.”
The national trend in health care is to deinstitutionalize and bring services to homes and communities. It is hoped that emphasizing prevention and healthy living will significantly reduce the need for hospitals, expensive drugs, surgery and high-tech equipment. The NDP has pledged to spend $647 million to reform long-term care services by 1997 – creating services that will allow seniors to stay in their own homes.
Problem is, the NDP has embarked on radical down-sizing of hospitals – closing beds and laying off thousands of health care workers – right now. Lankin claims that in the worst-case scenario, layoffs this year wouldn’t exceed 2,000, but the Ontario Hospital Association claims 14,000 jobs are in jeopardy. Phillips believes it will be hard to estimate job loss: “It is hard to even record the number of nursing jobs lost, because for every full-time job cut many part-time and relief positions go with it.”
Chaos will result when people who depend on hospitals have nowhere to turn but the inadequate community health care services, which are uneven and narrowly focussed. To make things worse, the same funding restrictions placed on hospitals have also hit the services that are supposed to save the day.
“I haven’t heard of any change in the quality of care. It is just too early,” says Phillips about the effect of layoffs on hospitals. “Right now the nurses are picking up the slack, but soon they will burn out. I don’t feel confident this government has the management skills to do this. I’d like to see a plan in place before moving people into the community.”
Training for laid-off hospital workers will have to come from the $160-million allocated for retraining workers laid off by cities, universities and school boards – all of whom are coping with record-low budget increases.
In February, Lankin appealed to hospitals to do everything in their power to make layoffs painless and to trim doctors and administrators first. But the NDP has yet to pass legislation that would bind hospital boards to make the right cuts. The boards operate at arm’s length from government and continue to make unnecessary decisions, ignoring the NDP’s moral pleas.
Rosana Pellizzari, a member of the Medical Reform Group and chair of the Ontario Association of Health Centres, wants better community accountability for hospitals before they lay off staff and cut services: “Sometimes it makes sense to bring people to hospitals. Planning must be at the community level and open and democratic. Health care workers, who are mostly women, should not be scapegoated for financial problems. Doctors and management should go first. Physicians experience very little unemployment.”
Carol Kushner, co-author of the book Second Opinion, which evaluates the country’s medical system, sees chaos resulting from the conflicting agendas of governments and health care reformers: “Will the tremendous contradictions of institutions be transferred to the community? The federal government is rapidly draining money from medicare while provincial governments are having a hard time. This hasn’t produced extra funds for re-allocating services to the community – which was recommended by reformers. You have to ask: who is going to fall through the cracks?”
A pioneering tool for gathering health data now being used in Kenya could herald a revolution in the way diseases are tracked and defeated around the world. It uses mobile phones to better connect patients with medical and health personnel, and allows data to be gathered in real-time and used to track health and improve the delivery of services, especially to remote and under-serviced areas.
In the past couple of years, Kenya has become a hotbed of mobile phone and information technology innovation. The now-famous Ushahidi crisis-mapping platform (www.ushahidi.com) is just one example. Social enterprise Data Dyne (www.datadyne.org) – with offices in Washington DC and Nairobi, Kenya – is offering its EpiSurveyor application (www.episurveyor.org) free to all to aid health data collection. It bills itself as “the first cloud-computing application for international development and global health … Think of it as like Gmail, but for data collection!”
EpiSurveyor claims to have more than 2,600 users around the world and is currently being upgraded to a second version.
“With the touch of a button I can see what’s going on across the country in real time,” Kenyan civil servant Yusuf Ibrahim told Britain’s Daily Telegraph newspaper. “It is amazing.”
Ibrahim works in Nairobi as the Kenyan Ministry of Health liaison to Data Dyne.
He uses maps and charts on mobile phones to track deadly disease outbreaks and vulnerable pregnancies.
The EpiSurveyor application works simply: A user logs into the website and builds and creates the sort of form they want. They then download it to a phone and start collecting data straight away.
Ibrahim gathers this data from mobile phones used by health care workers across the country.
“It used to take days, weeks or even a couple of months to find out about an outbreak of polio on the other side of the country,” he said. “Now we know almost instantly. The speed with which we can now collect information has catapulted healthcare and prevention to another level. It has completely changed healthcare and saved countless lives.”
He proudly points out Kenya’s mobile phone data collection system is “probably better than what they’ve got in the West.”
“Although we are a third world country, I’m pretty sure we’ve done this before
Western countries. While they are still collecting information in hard copy on clipboards, we are getting it instantly.”
Packed with data processing power, mobile phones are capable of an immense range of tasks and applications. Some see phones as key to a revolution in how healthcare is provided: the mobile phone becomes one-part clinic, another part mobile hospital dispensing advice and transmitting vital information back to healthcare professionals and scientists in hospitals and labs.
Despite dramatic improvements to the quality of hospitals in Africa and the number of qualified doctors, the continent’s healthcare services are still a patchwork, with rural and slum dwellers poorly served and the stresses of treating patients with contagious diseases like HIV/AIDS and malaria pushing resources to the limit.
The United Nations has a number of initiatives partnering with mobile phone manufacturers, networks and software developers as part of a global campaign to reduce HIV/AIDS, malaria and deaths in childbirth.
EpiSurveyor is being used by more than 15 countries’ ministries of health and is the adopted standard for the World Health Organization (www.who.int) (WHO) for electronic health data collection.
It began as a partnership with the United Nations Foundation, The Vodafone Group Foundation, WHO and the ministries of health of Kenya and Zambia in 2006 to pilot test the software for EpiSurveyor.
At the United Nations Foundation (www.unfoundation.org), chief executive Kathy Calvin equates the impact of mobile phones on global healthcare to the discovery of the antibiotic penicillin.
“Instead of building clinics and roads to remote towns and villages so that people can access healthcare, we are bringing healthcare directly to the people via mobile phones. You get a lot more healthcare for your money,” Calvin told the Telegraph.
Development Challenges, South-South Solutions was launched as an e-newsletter in 2006 by UNDP’s South-South Cooperation Unit (now the United Nations Office for South-South Cooperation) based in New York, USA. It led on profiling the rise of the global South as an economic powerhouse and was one of the first regular publications to champion the global South’s innovators, entrepreneurs, and pioneers. It tracked the key trends that are now so profoundly reshaping how development is seen and done. This includes the rapid take-up of mobile phones and information technology in the global South (as profiled in the first issue of magazine Southern Innovator), the move to becoming a majority urban world, a growing global innovator culture, and the plethora of solutions being developed in the global South to tackle its problems and improve living conditions and boost human development. The success of the e-newsletter led to the launch of the magazine Southern Innovator.














You must be logged in to post a comment.