It isn’t the nicest thing to think about, but if accident or illness strikes, you could end up receiving unwanted treatment.
But in 1994 things will change. The living will or advance directive – a document clearly stating a patient’s wishes about how they want to be treated – will become part of the doctor-patient relationship.
A trio of acts passed last December – the Advocacy Act, the Substitute Decisions Act and the Consent to Treatment Act – allow, albeit in rather vague language, for Ontarians to set out in advance which medical procedures they would or wouldn’t accept and let’s them name a proxy in case they are incapable of expressing their wishes.
This vague language – intended to allow patients to customize their wishes – means that writing a living will can prove to be a troubling and confusing experience.
To aid decision-making, the University of Toronto Centre for Bioethics is offering advice through a “model” living will.
The centre’s Dr. Peter Singer has geared the “model” to meet Ontario legislation and to offer a guide for anybody who doesn’t know where to begin.
“We put a lot of detail in the advance directive about states of incompetence people get into, and also the sorts of procedures providers might recommend in those health states.”
Singer sees living wills as an effective tool aiding patients to control their own health care.
“Unless the doctor is a longstanding friend it’s hard to know what patients want. As a practicing doctor, I have run into an incompetent person where their family member has no idea what sort of wishes the person would have wanted. The goal of a living will is to provide the personal care the patient would want.”
But there is a danger. Dr. Singer urges the need for informed and detailed language in a living will.
“If I have a couple minutes to make a decision I need a document that gives me a lot of confidence that this person wouldn’t want this treatment.”
In an emergency, the doctor might not even know of the living will’s existence. Dr. Singer advises giving a copy to your family doctor, lawyer, or proxy, and keep one with you at all times. When so-called “smart” health cards come along, Dr. Singer would like to see the living will recorded on the magnetic strip along with other health information.
Many of today’s seniors fought for Canada’s internationally-admired public health system. But more and more people are becoming worried that the combination of health care reform, funding cutbacks and free trade is fuelling the growth of a second tier of private medical services serving the well off.
The provincial government sees things differently, arguing Ontarians no longer expect government to pay for everything and rather than eroding medicare, the NDP is reinventing it.
Whichever way one looks at it, private insurance companies, homecare providers, labs and other services designed to make money are becoming more and more involved in the health care business.
Operating in the territory outside the guidelines of the 1984 Canada Health Act – which sets out the principles of medicare for the federal government to enforce – the private sector has room to expand, at the same time as OHIP coverage is scaled back from more and more services.
Janet Maher, whose Ontario Health Coaltion (OHC) represents doctors, nurses and other health care workers, worries for the future of medicare.
“A number of things like accommodation services – laundry, food services – are in the grey area of the Canada Health Act,” says Maher. “So with all these fees that are being introduced, by the strict letter of the law, there is no way to stop them. But as far as we are concerned the spirit of the Act isn’t being observed.”
In its current reforms, the government of Ontario is emphasizing paramedical professions like midwives who fall outside the CHA and aren’t covered by OHIP. The turn to community-based services means that people have to rely more on services and providers that aren’t covered under the CHA.
Maher says privatizing accommodation services is a recent phenomenon, the result of hospitals finding creative ways to trim their budgets.
“It’s a new area that hospitals are taking bids on,” she says. “The other thing around the accommodation services is that because they are not categorized, strictly speaking, as health care services, none of this is exempted in the Free Trade Agreement from U.S. competition.”
A recent report by two British Columbia researchers tries to put together this complex puzzle. Jackie Henwood and Colleen Fuller of the 7,500-member Health Sciences Association of British Columbia recently charged that a combination of free trade and budget-slashing governments is eroding the universality of medicare and ushering in a two-tier system.
Fuller and Henwood identify the Free Trade Agreement as the culprit. While the health care industry created more jobs than any other sector of the Canadian economy between 1984 and 1991, they point out the job growth has been concentrated in the private sector since free trade was implemented in 1989. And they expect worse under the proposed North American Free Trade Agreement (NAFTA).
“NAFTA will accelerate trends towards a privatized, non-union and corporate-dominated system of health care in Canada.”
One provision of the Free Trade Agreement has also made it possible for U.S. companies to compete against Canadian firms in health care. Chapter 14, “health-care facilities management services”, allows wide-open competition.
Under NAFTA, provisions will bind all levels of government to consider for-profit health care companies on both sides of the border on equal footing with public providers when bidding for services, and entitles them to compensation if they can prove to an arbitration board they’ve been wronged.
“That represents a substantial encroachment on the democratic right of local, provincial and federal governments to make decisions,” says Cathleen Connors, who chairs the national wing of OHC, the Canadian Health Coalition.
It’s this plus health care cutbacks – federal and provincial – that’s resulting in service and job cuts and bed closures in the public sector and an increase in privatization, say Henwood and Fuller. These opportunities have not gone unnoticed by private companies south of the border.
One such company is American Medical Security Inc. (AMS) of Green Bay Wisconsin. After hiring Canadian pollsters Angus Reid to do a survey, AMS saw a profitable market in offering American hospital insurance to frustrated Canadians awaiting surgery. Sixteen per cent of those polled said they wanted this service; that was enough for AMS.
“One thing that comes across loud and clear is that Canadians for the most part are happy,” says spokesperson Carrie Galbraith. “They know they are taken care of during an emergency. But they are willing to pay a little extra if they need care.”
So far, AMS offers its plan to Ontario, B.C. and Manitoba, with Toronto its best market. Galbraith says plans are in the works to expand to all of Canada except the territories.
Unfortunately, like most private health plans, AMS cuts its losses by avoiding what Galbraith calls “adverse selection” – anybody with a known serious health problem need not apply.
Here in Ontario, private for-profit home care services take in close to half of all OHIP billings. Many clients pay out of their own pockets for additional services.
The Ontario health ministry doesn’t keep statistics on the extent of the private home health care sector, says spokesperson Layne Verbeek. But the Ontario Home Health Care Providers’ Association, a trade group, estimates private homecare companies now employ 20,000 and serve more than 100,000.
“It’s a market situation,” says Henwood. “If the services aren’t available to people within the public sector, they will go outside of it. We’ve seen this in other countries like England, where they had a public system and now have a parallel private system. If you erode a system enough that people get angry, they are going to start to look for alternatives, and the people with the greatest liberty are those with money.”
But in a recent interview, health minister Ruth Grier was adamant this scenario wouldn’t be allowed to take place in Ontario. She strongly disagreed that medicare is being weakened due to recent changes, and said the government has actually “reaffirmed its commitment to medicare.”
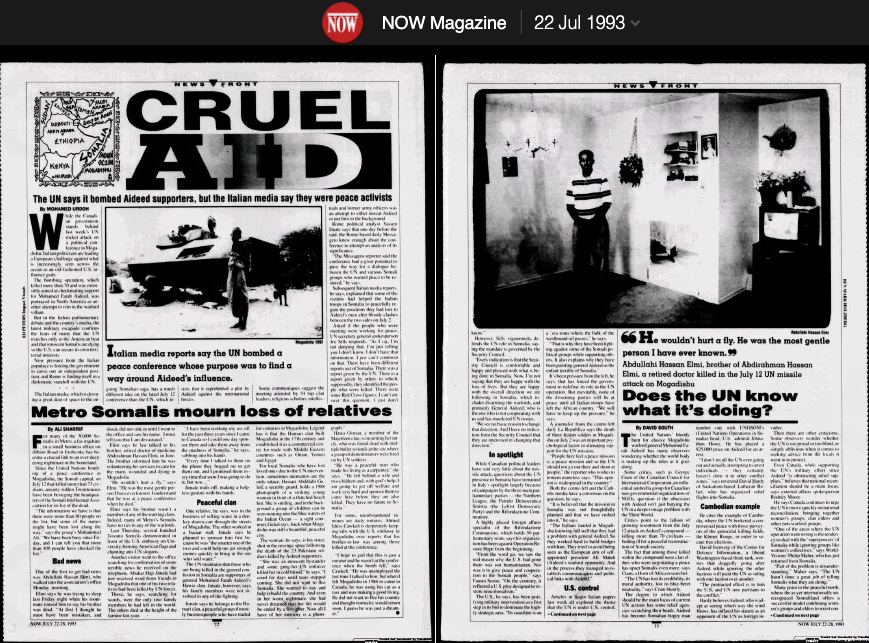
The United Nations’ bloody hunt for elusive Mogadishu warlord general Mohamed Farah Aideed has many observers wondering whether the world body is making up the rules as it goes along.
Some critics, such as George Cram of the Canadian Council for International Cooperation, an influential umbrella group for Canadian non-governmental organizations of NGOs, question if the obsession with Aideed isn’t just burying the UN in a deeper image problem with the Third World.
Critics point to the fallout of growing resentment from the July 12 attack on Aideed’s compound – killing more than 70 civilians – boding ill for a peaceful reconstruction of Somali society.
The fact that among those killed within the compound were clan elders who were negotiating a peace has upset Somalis even more, says Cram, a Horn of Africa researcher.
“The UN has lost its credibility, its moral authority, lost its blue-beret neutrality,” says Cram bluntly.
The degree to which Aideed should be the main focus of current UN actions has some relief agencies scratching their heads. Aideed has become Somalian bogey man number one with UNOSOM’s (United Nations Operations in Somalia) head, US Admiral Johnathon Howe. He has placed a $25,000 price on Aideed for an arrest.
“I don’t recall the UN ever going out and actually attempting to arrest individuals – they certainly haven’t done it in other conflict zones,” says reverend David Hardy of Saskatoon-based Lutheran Relief, who has organized relief flights into Somalia.
Cambodian example
He cites the example of Cambodia, where the UN brokered a controversial peace with those purveyors of the genocidal killing fields, the Khmer Rouge, in order to secure free elections.
David Isenverg of the Center for Defense Information, a liberal Washington-based think tank, worries that doggedly going after Aideed while ignoring the other factions will paint the UN as siding with one faction over another.
“The protracted effect is to turn the US and UN into partisans to the conflict.”
Hardy believes Aideed, who is adept at seeing which way the wind blows, has inflated his stature as an opponent of the UN as foreign invader.
Then there are other criticisms. Some observers wonder whether the UN is too proud or too blind, or simply oblivious when it comes to seeking advice from the locals it went in to protect.
Even Canada, while supporting the UN’s military effort since Aideed “is obstructing relief supplies,” believes that national reconciliation should be a main focus, says external affairs spokesperson Rodney Moore.
He says Canada continues to urge the UN to move quickly on national reconciliation, bringing together women’s groups, clan elders and other non-warlord groups.
“One of the areas where the UN operation went wrong is the tendency to deal with the ‘superpowers’ of Somalia while ignoring groups like women’s collectives,” says World Visions’ Philip Maher, who has just returned from Somalia.
“Part of the problem is misunderstanding,” Maher says. “The UN hasn’t done a great job of telling Somalis what they are doing.”
Many point to the peaceful north, where the as yet internationally unrecognized Somaliland offers a successful model, combining women’s groups and elders to wrest control.
“Does the UN know what it’s doing?”: Now Magazine, July 1993. This incident was the basis of the 2001 film Black Hawk Down.
Canada’s troubled airline industry is about to face some more turbulence, as the union representing more than 6,000 flight attendents presses its concern that many of its members’ health problems are related to poor air quality in jets.
The Canadian Union of Public Employees (CUPE) says its locals have compiled data that paints a fairly stale profile of in-flight air quality and its relationship to altitude, passenger load and length of flight. As part of the survey, the union recorded flight crews’ complaints of chest pains and lack of oxygen, as well as other work-related problems like back injuries, hearing loss and high incidence of colds and flu.
Of more interest to frequent fliers might be the opinion of some experts that even the more common jet lag may be caused by excess carbon dioxide, ozone and radiation. More than half the air in many aircraft is recirculated, “stale” air that is high in carbon dioxide and may be carrying bacteria and viruses, according to some experts.
CUPE health and safety chair Tracy Angles says the union now has enough evidence to at least pressure the carriers to undertake more comprehensive air quality studies. CUPE represents workers at Air Canada, Canadian, Nationair, Air Transat and some smaller feeder carriers.
While the union’s study is the first of its kind in Canada, a survey by the US department of industrial relations found, among other things, that flight attendents had 20 times the expected frequency of respiratory illness.
Flying mines
“Flight attendants have been equated with coal miners in terms of the bad air they have to breathe,” says Angles. “But this is not something the companies want to study.”
However, spokespeople for Air Canada and Canadian Airlines say they have not heard of such health problems. Jerry Goodrich of Canadian simply says, “It’s not an issue.”
However, while earlier-model jets supplied the cabin with 100 per cent fresh air, increasing fuel costs led to some modification. Modern jets mix fresh air – expensive to produce – with stale air from inside the cabin, which is passed through filters. The percentage of recirculated air in some aircraft, such as the popular Boeing 747-400, could be as high as 52 per cent, Boeing’s figures show.
Boeing’s Tom Cole says air circulation in Boeing’s jets is better than in an average office building, and that the passengers are “washed” with air to eliminate carbon dioxide and other hazards.
Critics like Georgia doctor William Campbell Douglass, publisher of the health newsletter Second Opinion, charge that the high rates of recirculated air, and the reliance on passengers’ own breath and perspiration to humidify the dry air, provide a perfect environment for bacteria and viruses. Douglass even speculates that planes could transmit serious diseases like tuberculosis. He suggests jet leg could be “nothing more than CO2 intoxification and oxygen starvation.”
“There is no doubt if you are in a confined space, you are at greater risk,” says University of Toronto microbiologist Eleanor Fish. “Aircraft filter systems aren’t sophisticated enough to filter out all the bacteria and viruses. But I’d be hard pressed to believe that you are at greater risk traveling on airplanes than on elevators.”
It is difficult for public health authorities to pin down the health risks of airplane travel because passengers disperse immediately after a flight. However, medical journals have documented two cases where virus transmission could be established because the passengers were easily traceable.
In 1977, 38 of the 54 passengers on a plane grounded in Alaska for a four and a half hours came down with the same strain of flu.
“We consistently hear complaints about certain aircraft,” says Angles. “The Airbus 320 is one of the worst.”
Angles says many airlines exacerbate the problem by over-crowding planes and flying them longer and farther than they were designed for.
Cut corners
“With deregulation, they have more people in there than was ever planned on. Nationair is a good example. A normal class Air Canada 747 carries about 420 people. In the all-economy configuration the load is upwards of 496.”
Angles also says airlines have been known to cut corners by turning down air flow to save money. In their 1990 book The Aircraft Cabin: Managing the Human Factors, Mary and Elwin Edwards cite a study indicating a 1 per cent saving on a fuel bill can be achieved by reducing the ventilation rate in a McDonnel-Douglas DC-10.
“A new global campaign and film asks whether the air we breathe on commercial flights is as safe as we think it is. …
Another issue, which frequently gets overlooked, is the quality of the air passengers breathe onboard
In February, a global campaign was launched by the Global Cabin Air QualityExecutive (GCAQE), which called for the mandatory introduction of effective filtration and warning systems, to be installed on all commercial passenger jet aircraft.
According to the GCAQE, there have been 50 recommendations and findings made by 12 air accident departments globally over the last 20 years, directly related to contaminated air exposures on passenger jet aircraft.
However, commercial aircraft continue to fly, with no contaminated air warning systems to inform passengers and crews when the air they are breathing is contaminated.”
“Particles the size of the new coronavirus are quickly purged from a commercial aircraft cabin, according to a U.S. Defense Department study touted by United Airlines Holdings Inc. in its effort to reassure wary travelers.
Filtration systems and rapid air-exchange rates mean that only about 0.003% of infected particles entered a masked passenger’s breathing zone, said the report, released Thursday.”
“On October 5, 2018, a 5-year FAA bill became law. Included in the bill is a study on technologies to combat contaminated bleed air. This is significant progress!”
“What does this tell us? Aerosols, very small particles of saliva containing the virus we exhale when we sneeze or even when we breathe if we have the flu, probably have an important role in the transmission of influenza. In addition to that we have public transportation, with a great number of people circulating in a place that may be closed and badly ventilated at times and we may have a notion of the importance of public campaigns that promote education and awareness of contaminated people to avoid leaving their homes when they have the flu and that they cover their mouth and nose with a disposable tissue when they sneeze and discard it right after that.”
“The revised International Health Regulations, adopted in 2005, provide a legal framework for a more effective coordinated international response to emergencies caused by outbreaks of infectious diseases. A number of provisions are relevant to the detection and control of TB during air travel, strengthening the authority of WHO and of national public health authorities in this domain. Because of these important developments since the original guidelines were issued in 1998, WHO has prepared this revised version to take account of current public health risks that may arise during air travel and new approaches to international collaboration in dealing with them. The guidelines were developed with the collaboration of international experts in air travel medicine and other authorities. Implementing the recommendations will help to reduce the spread of dangerous pathogens across the globe and decrease the risk of infection among individual travellers.“
“A Jet airliner with 54 persons aboard was delayed on the ground for three hours because of engine failure during a takeoff attempt. Most passengers stayed on the airplane during the delay. Within 72 hours, 72 per cent of the passengers became III with symptoms of cough, fever, fatigue, headache, sore throat and myalgia. One passenger, the apparent Index case, was III on the airplane, and the clinical attack rate among the others varied with the amount of time spent aboard. Virus antigenlcally similar to A/Texas/1/ (H3N2) was Isolated from 8 of 31 passengers cultured, and 20 of 22 ill persons tested had serologic evidence of infection with this virus. The airplane ventilation system was inoperative during the delay and this may account for the high attack rate.”
“At the end of its review of health data in the 1986 report The Airliner Cabin Environment: Air Quality and Safety, the National Research Council (NRC) committee concluded that “available information on the health of crews and passengers stems largely from ad hoc epidemiologic studies or case reports of specific health outcomes [and] conclusions that can be drawn from the available data are limited to a great extent by self-selection…and lack of exposure information” (NRC 1986). This chapter reviews data on possible health effects of exposure to aircraft cabin air that have emerged since the 1986 report and the emergence of data resources (e.g., surveillance systems) and studies that have particular relevance for the evaluation of potential health effects related to aircraft cabin air quality. Selected earlier sources are also reviewed. The decision to ban tobacco-smoking on domestic airline flights in 1987 and on flights into and out of the United States in 1999 reduces the relevance of some studies of exposures and reported signs and symptoms that clearly could have been related to the products of tobacco smoke.”










You must be logged in to post a comment.